-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
-
Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
May 2024
Gastric biopsy from a patient with liver cirrhosis.

Diagnosis
Poorly cohesive (“diffuse”) gastric adenocarcinoma with foamy (histiocyte-like) cells.
Comment
An oesophagogastroduodenoscopy was performed in a 57-year-old male patient with previously known liver cirrhosis and consequent portal hypertension gastropathy. Upon endoscopy, the clinicians described a gastric ulcer located in the distal corpus. Biopsies were taken from the lesion.
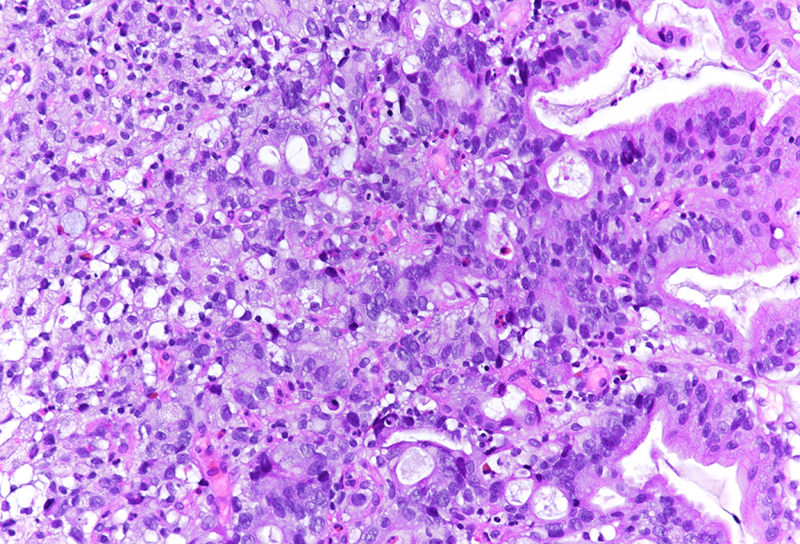
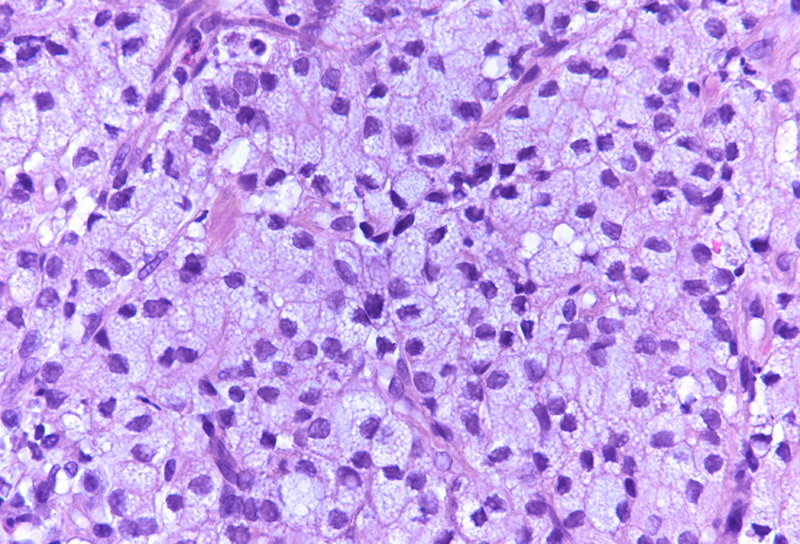
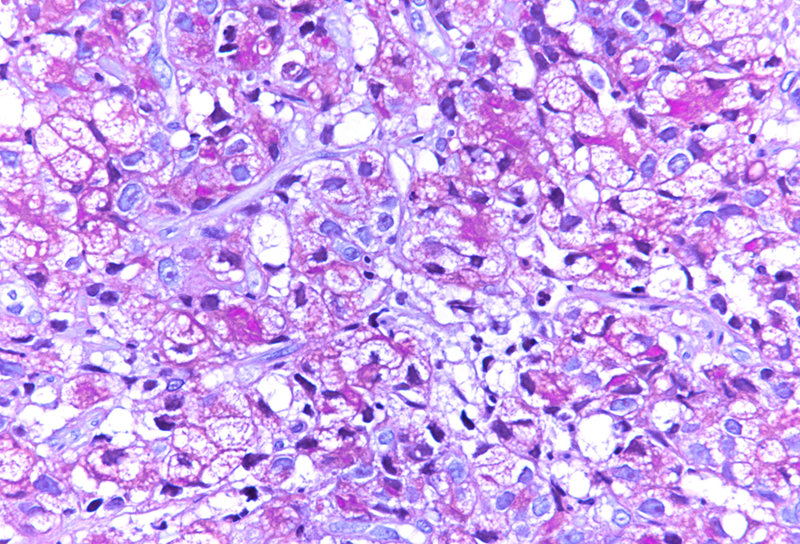
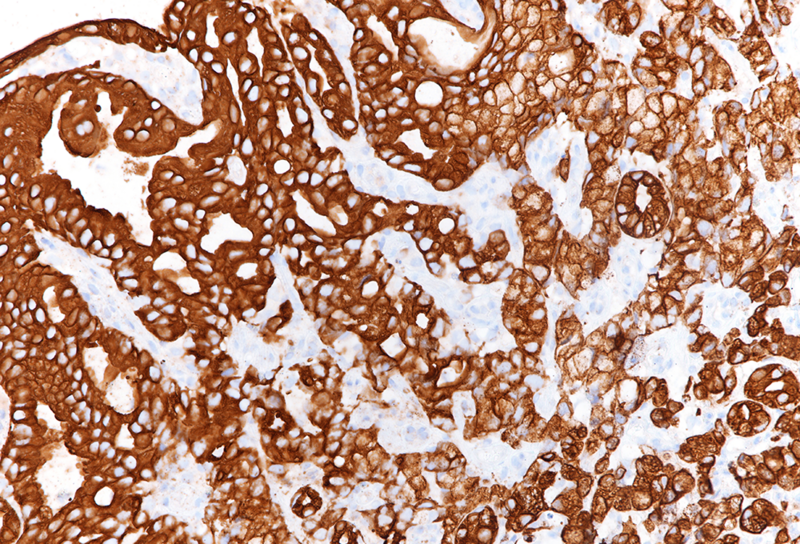
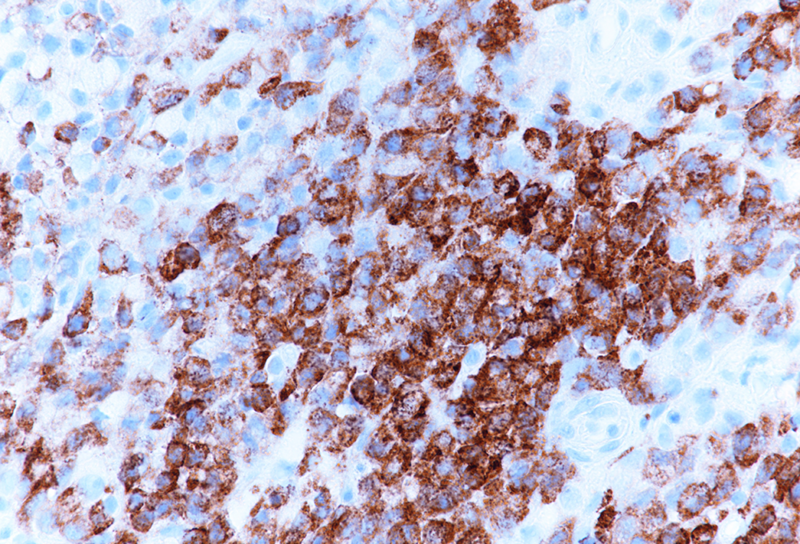
Histologically, we saw two biopsy pieces with gastric mucosa. On the first one, there was a normal corpus mucosa with no inflammation, no atrophy and no intestinal metaplasia. However, on the second one, there was a dense infiltrate of cells with ample foamy cytoplasm, yet only slightly enlarged, hyperchromatic nuclei, which were placed either centrally or eccentrically, that is, close to the cellular membrane. Occasional classical signet ring cells were also present (Panels A-B). The foamy cells were weakly positive for PAS (Panel C), albeit diffusely positive for pankeratin (Panel D). We performed some additional stains: The foamy cells were positive for MUC5AC (Panel E) and MUC6 (Panel F), while negative for MUC2 (not shown). A final diagnosis of poorly cohesive (“diffuse” according to Lauren) gastric adenocarcinoma with foamy (histiocyte-like) cells.
There are two widely used morphological classifications of gastric cancer, WHO and Lauren classification. Lauren classification divides gastric cancer in intestinal and diffuse type, the latter being subdivided into signet-ring cell (SRC) subtype and poorly cohesive carcinoma-not otherwise specified (PCC-NOS). PCC-NOS is a heterogeneous group of morphological descriptions of gastric carcinoma, but, so far, with merely academic and no significant clinical relevance.
The presented case demonstrates tumour cells, which could easily be mistaken for histiocytes, in particular since classical PAS-positive signet ring cells were only focally present. As in a benign histiocytic proliferation, e.g. in a xanthelasma, the nuclei of the tumour cells were not markedly enlarged, often centrally placed, still slightly irregular and hyperchromatic. The keratin stain definitively made the diagnosis.
For further reading
- Chiaravalli AM, Klersy C, Tava F et al: Lower- and higher-grade subtypes of diffuse gastric cancer. Hum Pathol. 2009 Nov;40(11):1591-9
- Murakami H, Nakanishi H, Tanaka H et al: Establishment and characterization of novel gastric signet-ring cell and non-signet-ring cell poorly differentiated adenocarcinoma cell lines with low and high malignant potential. Gastric Cancer. 2013 Jan;16(1):74-83
- Kwon CH, Kim YK, Lee S et al: Gastric poorly cohesive carcinoma: a correlative study of mutational signatures and prognostic significance based on histopathological subtypes. Histopathology. 2018 Mar;72(4):556-568.
- Garcia-Pelaez J, Barbosa-Matos R, Gullo I, Carneiro F, Oliviera C: Histological and mutational profile of diffuse gastric cancer: current knowledge and future challenges. Mol Oncol. 2021 Nov;15(11):2841-2867
- Yeo MK, Kang SH, Jeong KB et al: Comparison of Gene Expression Profiles of Signet Ring Cell Carcinoma and Poorly Cohesive Carcinoma in Early Gastric Cancer. Clin Med Insights Oncol. 2022 May 18:16:11795549221097941.
Presented by
Dr. Sara Hrg, Zagreb, Croatia, Dr. Cord Langner, Graz, Austria.
