-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
-
Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
June 2023
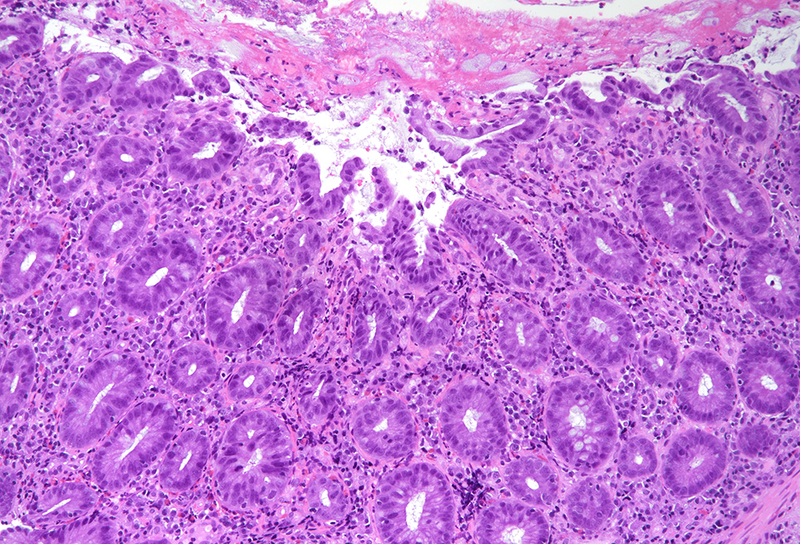
Colonic biopsy from a 62-year-old male.





Diagnosis
Amoebic colitis.
Comment
A 62-year-old male patient attends his physician for unspecific abdominal pain for two months. The symptoms had started with sudden-onset diarrhoea, successfully treated with antibiotics. No contact with animals or trips abroad were known/mentioned in the clinical record. Laboratory tests were unremarkable. No stool testing was performed. Colonoscopy showed erosions and ulcers with 2-4 cm of diameter covered with fibrin, in the cecum and transverse colon. Multiples biopsies were taken.
Histology revealed colonic mucosa with preserved architecture. Multiple erosions, crypts with degenerative features and increase of the inflammatory cell infiltrate in the lamina propria, especially granulocytes, were observed (PANEL A-B). On the luminal surface, accompanied by fibrin and debris, multiple organisms with roundish shape, foamy cytoplasm and round, pale and eccentric nuclei were found; some of those have erythrocytes engulfed in their cytoplasm (PANEL C-D); periodic acid-Shiff (PAS) stain highlights these organisms (PANEL E-F), which qualify for diagnosis of amoebiasis.
Intestinal amoebiasis is caused by the protozoan parasite Entamoeba histolytica. The prevalence is disproportionately much more common in developing countries than in developed nations, due to poor sanitation and low-socioeconomic status. In Western countries, this infection is usually seen in overseas travellers, immunocompromised patients, and institutionalized individuals. Internationally, amoebic colitis is the second leading case of death by a parasitic disease, with a mortality rate of approximately 100 000 deaths per year due to amoebic liver complications.
Amoebiasis spreads through ingestion of contaminated water or food, and it also can be spread by a faecal-oral route; sexual transmission has been reported sporadically. The parasitic cysts are resistant to gastric acid and the trophozoites are released in the small bowel, invading the intestinal crypts. The clinical spectrum of intestinal amoebiasis ranges from an asymptomatic carrier or with just only vague gastrointestinal symptoms to a severe fulminant necrotizing colitis with bleeding, perforation, and hematogenous dissemination to other organs, particularly to the liver. Fever, abdominal pain, tenesmus, and bloody or non-bloody diarrhoea are the usual symptoms.
The cecum is the most common site of involvement within the large bowel, followed by the right colon and rectum. Colonoscopy findings may be normal, especially in patients with mild disease. Most cases however show irregular shaped ulcers (“flash-shaped” lesions) and erosions with surrounding erythema, sometimes covered by a whitish exudate; the mucosa, between the ulcers or erosions, is usually normal.
Histologically, initial lesions show a mild neutrophilic infiltrate, with numerous organisms present at the luminal surface associated with detritus. In advanced disease, ulcers are often deep, extending into the submucosa, sometimes with invasive amoebae within the bowel wall. Entamoeba histolytica has a roundish shape, with foamy cytoplasm and round, pale and eccentric nuclei with an open nuclear chromatin pattern. Within the inflammatory exudate, they may be difficult to distinguish from macrophages; in these cases, histochemical and immunohistochemical stains may be performed: amoebae are trichrome- and PAS-positive and macrophages stain with CD68. It is noteworthy the presence of ingested erythrocytes as pathognomonic feature of this parasite.
For further reading
- Yue B, Meng Y, Zhou Y, et al. Characteristics of endoscopic and pathological findings of amoebic colitis. BMC Gastroenterol. 2021 Oct 9;21(1):367.
- Guillén N. Pathogenicity and virulence of Entamoeba histolytica, the agent of amoebiasis. Virulence. 2023 Dec;14(1):2158656.
- Wang H, Kanthan R. Multiple colonic and ileal perforations due to unsuspected intestinal amoebiasis – Case report and review. Pathol Res Pract. 2020 Jan;216(1):152608.
- Rahadiani N, Habiburrahman M, Putranto AS, et al. Fulminant necrotizing amoebic colitis presenting as acute appendicitis: a case report and comprehensive literature review. J Infect Dev Ctries. 2022 Apr 30;16(4):717-725.
Presented by
Dr. Rafael Moiteiro da Cruz, Lisbon, Portugal, and Dr. Cord Langner, Graz, Austria.
