-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
-
Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
July 2022
Ultrasound-guided biopsy of a pancreatic mass in a 51-year-old male.







Diagnosis
Poorly to undifferentiated carcinoma, with abortive glandular and squamous differentiation (consistent with adenosquamous carcinoma).
Comment
The patient presented with unspecific upper abdominal pain, raising suspicion for gastric ulcer. Gastroscopy was performed and was unremarkable. Computed tomography was performed and showed a mass lesion within the body of the pancreas, measuring 5.2 cm x 3.9 cm x 3.6 cm. Within the liver four lesions, measuring 1.2 cm in maximum diameter, were identified, suspicious of tumour metastasis. Endoscopic ultrasound and fine-needle aspiration biopsy (EUS-FNA) was performed.
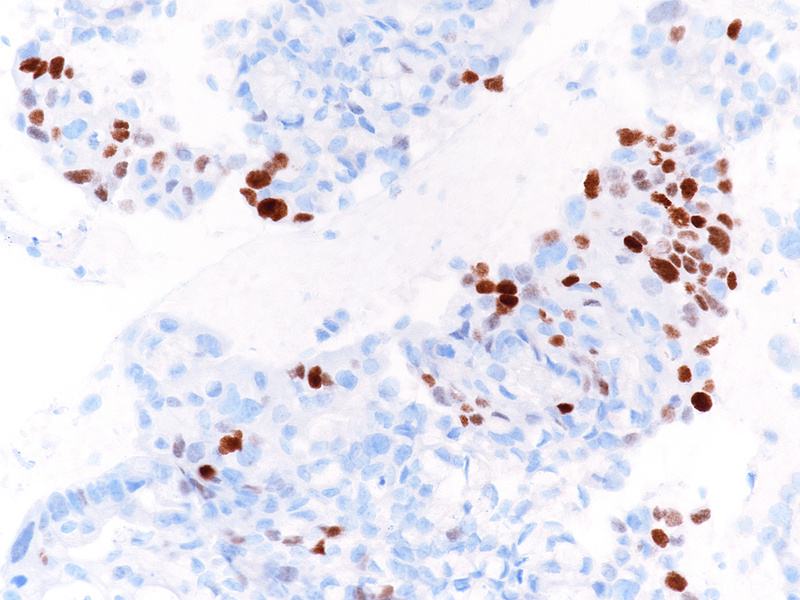
The well-sampled biopsy showed fragments of a necrotising carcinoma, arranged in isolated cells, small aggregates of cells and poorly formed glandular structures (Panels A-B). The tumour cells demonstrated abundant eosinophilic cytoplasm and severely pleomorphic, hyperchromatic nuclei with distinct nucleoli. Brisk mitotic activity was noted (Panel C). Within some clusters, the neoplastic cells had a more polygonal appearance, with intercellular desmosomes, more basophilic cytoplasm and evidence of dyskeratosis (Panels D-E).
By immunohistochemistry, the tumour cells were strongly and diffusely positive for CK7 (Panel F), focally positive also for p40 (Panel G) and CK20 (not shown). Ki67 labelling index confirmed the suspected high proliferation rate, estimated between 40-50% (Panel H). The immunohistochemical screening for DNA mismatch repair (MMR) deficiency showed no loss of protein expression. A final diagnosis of poorly (to undifferentiated) adenocarcinoma of the pancreas with squamous differentiation (consistent with adenosquamous carcinoma) was made.
EUS-FNA allows a diagnosis of pancreatic lesions with minimal invasive sampling. EUS-FNA for pancreatic lesions and suspected lymph node metastasis can confirm a diagnosis in cases with equivocal imaging results and allows for early therapy management of patients with non-resectable pancreatic masses. In borderline resectable cases undergoing neoadjuvant treatment, EUS-FNA is the sampling method of choice to avoid needle-track seeding outside the operation area.
A diagnosis of pancreatic ductal adenocarcinoma depends on architectural features (irregular distribution of cells within sheets and clusters of various sizes and irregular glandular shapes; glandular rupture; the presence of isolated cells) and cytological aspects (anisonucleosis; irregular nuclear membranes; heterogeneity of chromatin; frequent and/or atypical mitosis). If stroma is present, it usually shows a desmoplastic response.
Sometimes, EUS-FNA renders cytological material only. In these cases, the standardized terminology and nomenclature for pancreatobiliary cytology of the Papanicolaou Society of Cytopathology should be applied (Pitman et al. 2014).
Adenosquamous carcinoma accounts for only 0.4-4% of pancreatic adenocarcinomas; it has arbitrarily been defined as an adenocarcinoma combined with at least 30% of squamous component (WHO classification). However, any degree of squamous differentiation in a pancreatic carcinoma has been associated with a basal genomic profile and a poorer prognosis compared with pancreatic ductal adenocarcinoma - as such, a squamous component should always be included in the pathology report.
The study of microsatellite instability has been increasingly requested for patient management, as it indicates different responses to chemotherapy and potential benefit from immunotherapy by PD-1 blocking.
For further reading
- Pitman MB, Centeno BA, Ali SZ, Genevay M, Stelow E, Mino-Kenudson M, Castillo CF, Schmidt CM, Brugge WR, Layfield LJ. Standardized terminology and nomenclature for pancreatobiliary cytology: The Papanicolaou Society of Cytopathology Guidelines. Cytojournal. 2014 Jun 2;11(Suppl 1):3. doi: 10.4103/1742-6413.133343. eCollection 2014.
- Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, Lu S, Kemberling H, Wilt C, Luber BS, Wong F, Azad NS, Rucki AA, Laheru D, Donehower R, Zaheer A, Fisher GA, Crocenzi TS, Lee JJ, Greten TF, Duffy AG, Ciombor KK, Eyring AD, Lam BH, Joe A, Kang SP, Holdhoff M, Danilova L, Cope L, Meyer C, Zhou S, Goldberg RM, Armstrong DK, Bever KM, Fader AN, Taube J, Housseau F, Spetzler D, Xiao N, Pardoll DM, Papadopoulos N, Kinzler KW, Eshleman JR, Vogelstein B, Anders RA, Diaz LA Jr. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science. 2017 Jul 28; 357:409-413.
- Moslim M, Lefton M, Ross E, Mackrides N, Reddy S. Clinical and Histological Basis of Adenosquamous Carcinoma of the Pancreas: A 30-year Experience. Journal of Surgical Research. 2021; 259:350-356.
Presented by
Dr. Ana Varelas, Porto, Portugal, and Dr. Cord Langner, Graz, Austria.
