-
Die Universität
- Herzlich willkommen
- Das sind wir
- Medien & PR
-
Studium
- Allgemein
- Studienangebot
- Campusleben
-
Forschung
- Profil
- Infrastruktur
- Kooperationen
- Services
-
Karriere
- Arbeitgeberin Med Uni Graz
- Potenziale
- Arbeitsumfeld
- Offene Stellen
-
Diagnostik
- Patient*innen
- Zuweiser*innen
-
Gesundheitsthemen
- Gesundheitsinfrastruktur

Case of the Month
February 2023
Exophytic oesophageal tumour mass in an 84-year-old male.


Diagnosis
Mixed neuroendocrine-non-neuroendocrine neoplasm (miNEN).
Comment
84-year-old male presented with dysphagia and weight loss. Endoscopy revealed an exophytic lesion within the distal oesophagus (32-38 cm).
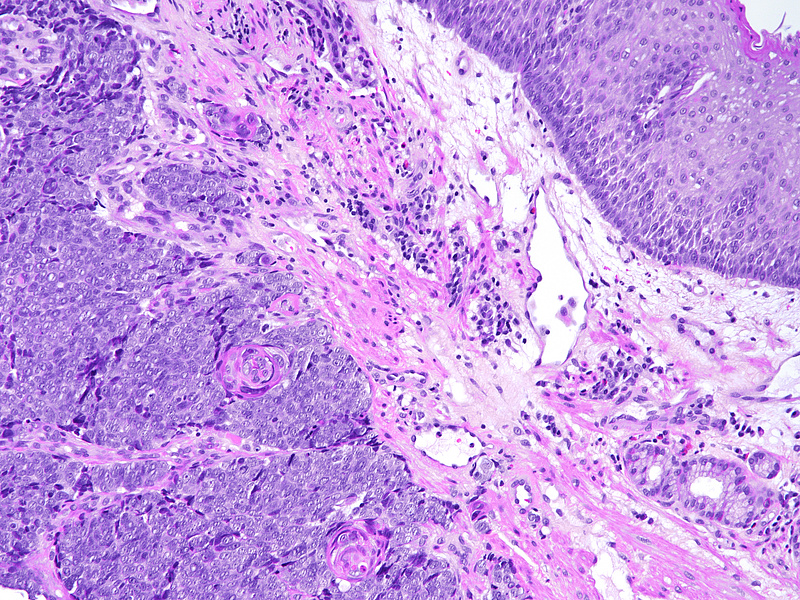
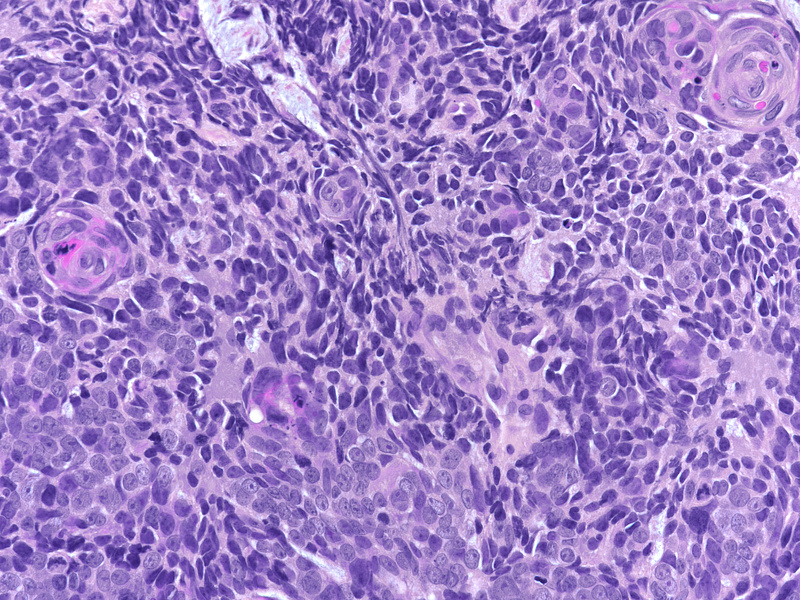
On low power the lesion is composed of sheets of monomorphic, overlapping small to medium sized malignant cells with irregular nuclear contours and finely dispersed chromatin without well-formed nucleoli (Panels A-B). Within these sheets of cells are demarcated areas of squamous differentiation, with formation of clearly visible squamous eddies and focal high-grade cytology (Panels C-D).
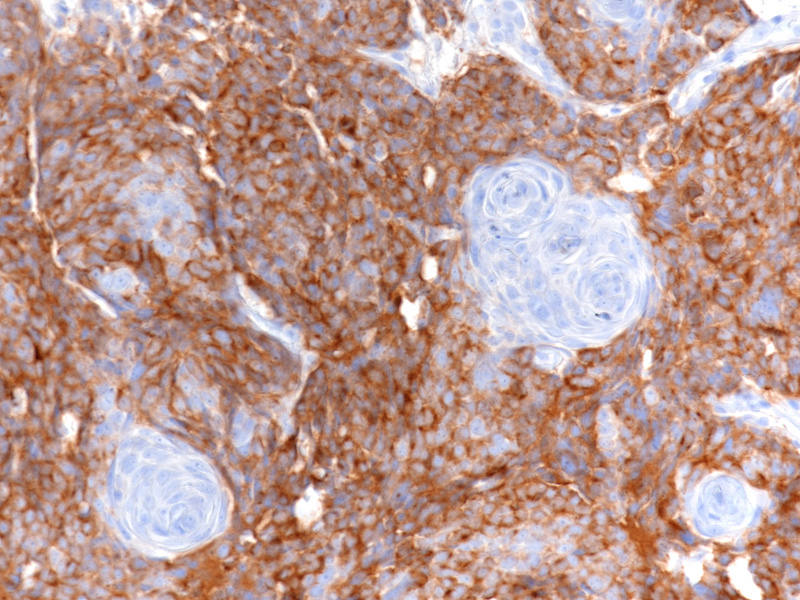
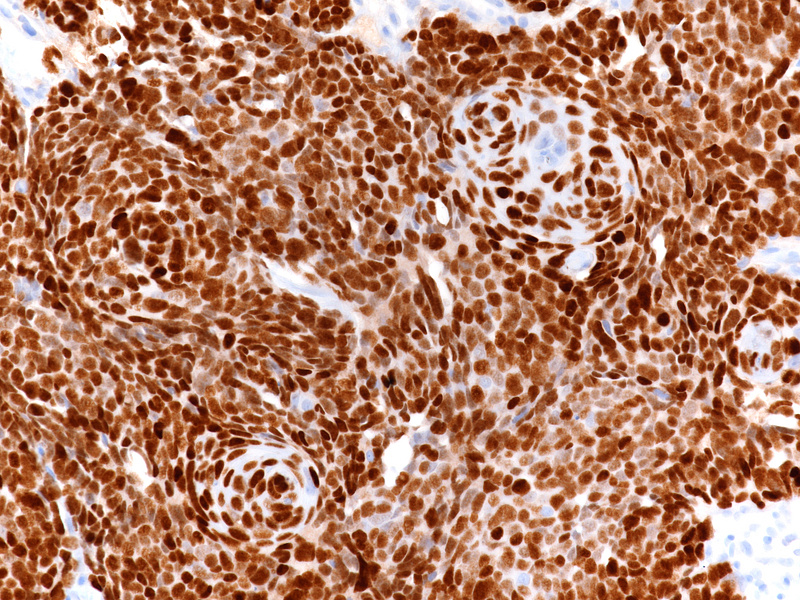
The immunohistochemical staining shows that the sheets of monomorphic cells show immunoreactivity for CD56 and synaptophysin (Panel E) and have a high proliferation index on ki67 staining (Panel F) proving neuroendocrine differentiation (neuroendocrine carcinoma, NEC). Of note, both areas of neuroendocrine and squamous differentiation show diffuse nuclear p40 immunoreactivity (Panel G) while cytokeratin positivity with CK5/6 is restricted to areas of squamous differentiation visible already on H&E, indicating more mature cells (Panel H). This reciprocal immunoprofile, taken together with the biphasic morphological pattern described above, is that of a mixed neuroendocrine-non-neuroendocrine neoplasm (miNEN).
miNEN is an umbrella term used to describe neoplastic lesions (NEN) encompassing gastric epithelial neoplasms with neuroendocrine differentiation mixed with a non-neuroendocrine neoplasm such as the squamous cell carcinoma in this instance. Oesophageal miNENs are usually composed of a poorly differentiated neuroendocrine carcinoma (NEC) and either a squamous cell carcinoma or an adenocarcinoma arising in either Barrett mucosa or ectopic gastric mucosa. Indeed, a case report has also demonstrated a trilineage lesion where both adenocarcinoma and squamous cell differentiation exist within the non-neuroendocrine component (1). It should be noted that collision tumours do not meet the definition of a miNEN. MiNENs often present with non-specific gastrointestinal symptoms relating to gastric bleeding (if there is tumour-related ulceration) or obstruction. Although incidence of these lesions is increasing in the USA and European populations, they remain rare and as a result, the underlying pathogenesis is largely unknown. Whilst few data are available, complex genetic factors such as chromosomal abnormalities affecting genes involved in cell-cycle dynamics are thought to play a prominent role (2).
In these lesions, the neuroendocrine component often has a high proliferative index (ki67 >55%), with an associated higher risk of metastasis (3) and shows immunoreactivity for the neuroendocrine markers such as CD56, synaptophysin and chromogranin A, as can be seen in our case. The non-neuroendocrine component, in our case, shows positivity for p40 and cytokeratin, the immunoprofile of a squamous cell carcinoma. Prognosis is largely dependent upon grade and stage, with grading using the same system for other gastroenteropancreatic neuroendocrine neoplasms.
For further reading
- Farooq F, Zarrabi K, Sweeney K, Kim J, Bandovic J, Patel C, Choi M. Multiregion Comprehensive Genomic Profiling of a Gastric Mixed Neuroendocrine-Nonneuroendocrine Neoplasm with Trilineage Differentiation. J Gastric Cancer. 2018 Jun;18(2):200-207.
- Makuuchi R, Terashima M, Kusuhara M, Nakajima T, Serizawa M, Hatakeyama K, Ohshima K, Urakami K, Yamaguchi K. Comprehensive analysis of gene mutation and expression profiles in neuroendocrine carcinomas of the stomach. Biomed Res. 2017;38(1):19-27.
- Zhang P, Li Z, Li J, Li J, Zhang X, Lu Z, Sun Y, Li Y, Zhou J, Wang X, Peng Z, Shen L, Lu M. Clinicopathological features and lymph node and distant metastasis patterns in patients with gastroenteropancreatic mixed neuroendocrine-non-neuroendocrine neoplasm. Cancer Med. 2021 Jul;10(14):4855-4863.
Presented by
Dr. Jenna Gregory, Aberdeen, Scotland, UK, Dr. Michael Mayr, Vienna, Austria, and Dr. Cord Langner, Graz, Austria.
